PCOS Renamed PMOS: The Long-Overdue Reframe in Women’s Reproductive Health
In a newly-published article by the Lancet (2025), the women’s health condition previously known as PCOS (Polycystic Ovary Syndrome) has been formally reclassified as ‘PMOS,’ or Polyendocrine Metabolic Ovarian Syndrome.1 This name change was the result of a multistep global consensus, established with engagement of 56 leading academic, clinical, and patient organizations, and more accurately reflects the disease’s multisystem pathophysiology.1
Why is the change from PCOS to PMOS so important?
It was never just about the cysts. The problem with the previous name, Polycystic Ovary Syndrome, is that it placed the pathological burden on ovarian cysts- which not every woman with ‘PCOS’ even experiences- and completely overlooked the diverse endocrine and metabolic features of the condition. This narrow focus was an incredible disservice to millions of women suffering from the disease because it frequently led to delayed diagnosis, fragmented care and significant stigma around associated symptoms like obesity and hyperandrogenism. Approximately 10% to 13% of reproductive age women around the world are impacted by PMOS, but an estimated 70% don’t know they have it- often because their symptoms seem unrelated to a reproductive disorder.2
The physiological complexity of PMOS results in not just menstrual irregularities and fertility challenges, but also insulin resistance, Type II Diabetes, obesity, cardiovascular disease, sleep apnea, depression, body dysmorphia and female-pattern baldness. Recognizing that this condition is not isolated to the ovaries and opening the range of diagnostic criteria is a huge step forward in improving diagnostic criteria and women’s health care.
PCOS: A brief history
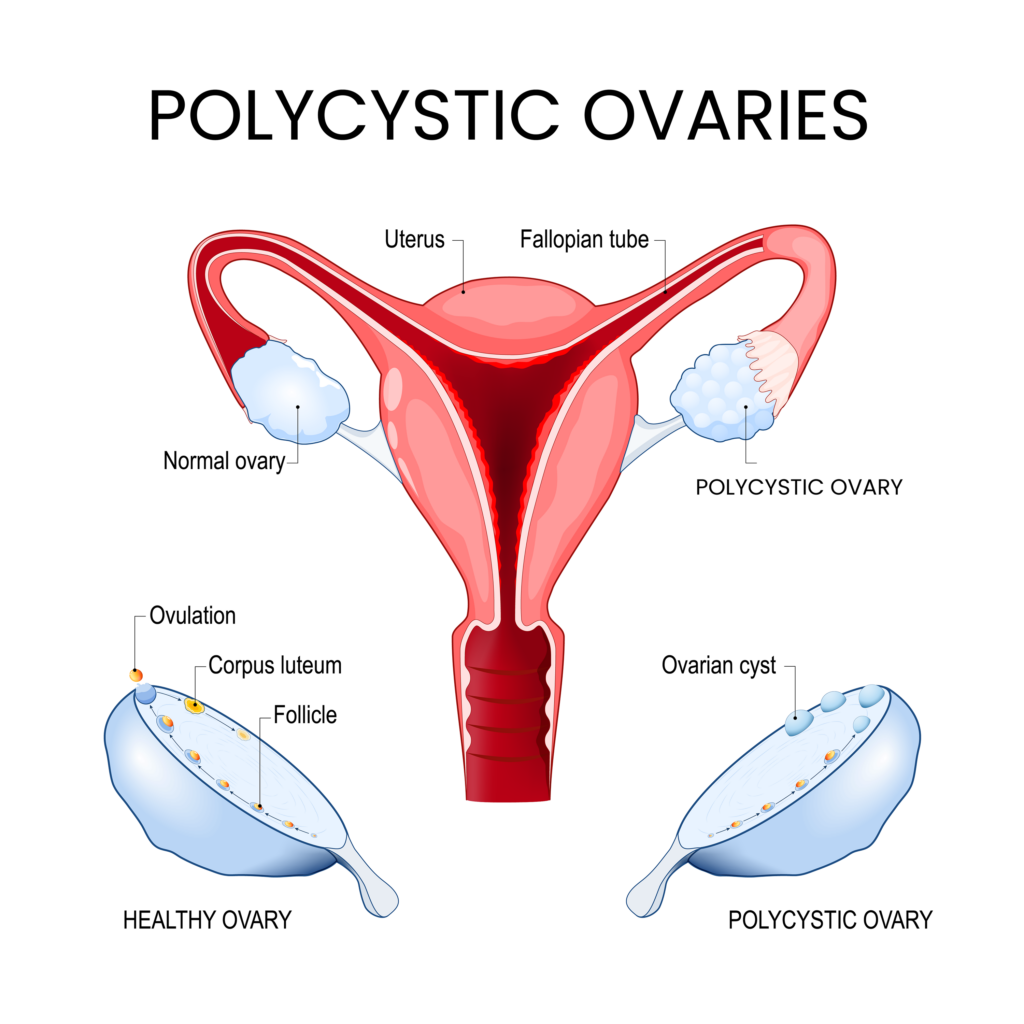
Prior to this reclassification and expansion of diagnostic criteria, PCOS was viewed in the medical community as primarily a gynecological or ovarian disorder, assumed to be relatively localized to menstrual and reproductive challenges. The term ‘polycystic ovary’ implies the presence of problematic or pathological cysts in the ovary, which are not truly a feature of the condition. Instead of dangerous or harmful cysts, the condition actually causes an accumulation of multiple small, harmless “follicles” (tiny, fluid-filled sacs that hold immature eggs). The predominant diagnostic for the condition has been the Rotterdam criteria, which diagnosis the disorder based on a) hyperandrogenism, b) oligo or anovulation, and c) the presence of polycystic ovaries. 3 This diagnostic criteria, however, overlooked women whose predominant symptoms manifested as metabolic irregularities, nervous system dysfunction or other hormone imbalances alongside menstrual irregularities or while maintaining relatively normal menstrual function.
From PCOS to PMOS: What the new name means
The new name more broadly captures the system-wide condition involving hormones, metabolism and ovarian function, and provides a clear picture of what is truly happening in the body:
Polyendocrine
The condition involves reproductive hormones like estrogen, progesterone and androgens (testosterone), but is not isolated to those hormones. It also involves metabolic hormones like insulin and neuroendocrine hormones like cortisol, highlighting the strong connection between PMOS and mood disorders like anxiety and depression.
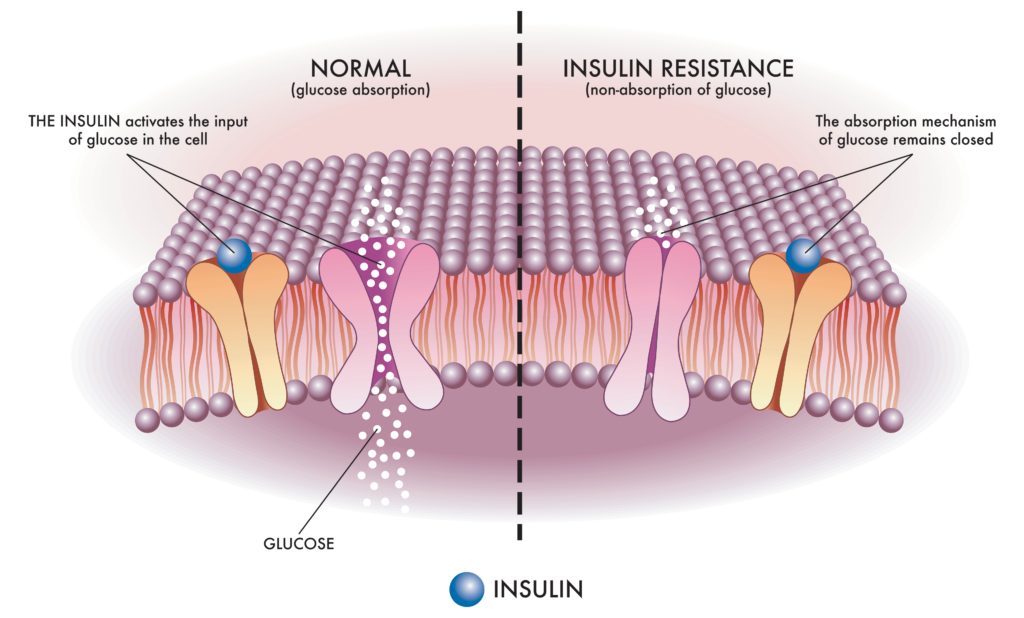
Metabolic
Insulin resistance is a foundational feature of this condition, and influences not just a predisposition to overweight and obesity, but a higher risk for dyslipidemia and cardiovascular disease- emphasizing the cardiometabolic burden of the disease.4
Ovarian
Disrupted ovarian function does remain a core tenet of PMOS, however the emphasis on the presence of ovarian cysts is no longer the feature of focus. Ovarian involvement is more heavily weighted on anovulation, irregular cycles, elevated LH:FSH ratio and fertility challenges. The key takeaway, however, is that ovarian dysfunction is recognized as part of the story, not the entire of the story.
Labwork for PMOS
For women showing up with challenges around weight management, mood and/or sleep disturbance, stress sensitivity, energy management concerns, acne and menstrual irregularities, these features widen the diagnostic lens away from the presence (or lack thereof) of ovarian cysts on an ultrasound. Comprehensive lab work to assess fasting insulin and glucose, hemoglobin A1C (HbA1C), androgen levels, estrogen, progesterone, luteinizing hormone, follicle stimulating hormone and a lipid panel can all be included to pinpoint the root cause to the disruption of metabolic, endocrine and Hypothalamic-Pituitary-Ovarian (HPO) Axis function that occurs with the PMOS story.
Holistic and Integrative PMOS management and interventions
Reframing the condition to a whole-body perspective elevates the scope of focus out of just the reproductive tract and into systemic management, prioritizing interventions that support endocrine regulation, metabolic homeostasis and nervous system stability.
Diet to Support PMOS

From a dietary perspective, the Mediterranean diet (MD), particularly one that is low glycemic, has been shown to be incredibly beneficial for women with PMOS through supporting insulin sensitivity, reducing the inflammatory load, and providing healthy fats for hormone function/balance.5 Periodic adherence to a ketogenic diet (KD) is also an excellent strategy for improving insulin response, reducing body weight and even reducing androgen dominance6– however long-term adherence to a KD diet may not be ideal from a mental health and sustainability perspective, so alternating a few months at a time on a KD diet with longer-term adherence to an MD diet provides a sustainable framework for a nutrition foundation grounded in multisystem balance.
Supplements: Herbs and Nutrients to Support PMOS
Certain targeted nutrients and botanicals can also fit within this multisystem framework to support the complex hormonal and metabolic picture of PMOS:
Myo-inositol is a type of sugar molecule involved in insulin signaling, the metabolizing of carbohydrates and fats, and the production of certain hormones. In women with PMOS, myo-inositol administered for at least 24 weeks was shown to improve their metabolic profile and reduce hyperandrogenism.7

If consuming enough omega-3 fatty acids through the diet is challenging, supplementing with a high-quality omega 3 oil can be an excellent way to support hormone health and manage the inflammation associated with PMOS. Supplementing with omega-3 fatty acids has been shown to reduce androgen levels,8 improve insulin resistance9 and reduce cardiometabolic risk,10 all features associated with PMOS.

Berberine, an alkaloid found in many bitter plants including Oregon grape root and phellodendron, has been shown in numerous studies to improve insulin receptor expression and glucose uptake 11. Studies have also shown that berberine is able to mitigate many of the key features of PMOS, including reducing testosterone and FAI, increasing SHBG, and mitigating the clinical symptoms of androgen excess, including hirsutism and acne.12

White peony root (Paeonia lactiflora) has been used in Traditional Chinese Medicine (TCM) for thousands of years as a treatment for gynecological disorders. While the exact mechanism of action is unknown, the constituent paeoniflorin has been shown in pre-clinical studies to regulate hormone production, improve ovarian fibrosis, reduce inflammatory parameters, and modulate aromatase activity to improve follicle development. 13,14
The combination with licorice root, a formula known as Shakuyaku-Kanzo-To in traditional Japanese medicine, has been used to regulate hormone production, particularly androgens 15. In addition to its estrogen-modifying and anti-inflammatory effects, licorice is also considered an adaptogen, making it a powerful ally in supporting the stress-response pathway within the PMOS paradigm.16

Gymnema, known in Ayurvedic medicine as ‘the sugar destroyer,’ is a powerful herb for supporting insulin sensitivity and even modifying sugar cravings. Gymnemic acids, one of the key classes of phytochemicals in the leaf, improve the ability of the pancreas to secrete insulin and lower both fasting and post-prandial (after meal) glucose levels.17 Those amazing gymnemic acids even bind to sweet taste receptors on the tongue, reducing the ability to taste sweetness and curbing sugar cravings.18 This is an especially important effect for helping with the sweet cravings that often accompany metabolic dysregulation in conditions like Type 2 Diabetes and PMOS.

Saw palmetto is another herb that has a long history of use in supporting both male and female reproductive health. The berries have been shown to inhibit the 5-alpha-reductase enzyme, which is responsible for converting testosterone into its more potent form, dihydrotestosterone (DHT).21 This results in an anti-androgenic effect that herbalists rely on for addressing many of the key features of PMOS, including androgenic alopecia (thinning hair), hirsutism and hormonal acne. Animal studies using a PMOS model have shown that Saw Palmetto reduced prolactin elevation and normalized follicle-development,22 actions that support ovulation regularity.
Magnesium plays a critical role in glucose metabolism; low magnesium intake/status can worsen insulin resistance, which individuals with PMOS are already at a higher risk of experiencing. Clinical research shows that supplementing with magnesium is able to improve insulin sensitivity, lipid profiles and glucose handling in individuals with PMOS,23 and may also have the benefit of alleviating pain and inflammation associated with PMOS-related menstrual challenges.

Cruciferous vegetables like kale, Brussels sprouts, broccoli and Spanish black radish contain compounds called glucosinolates, which modulates estrogen pathways by promoting the metabolism of active estrogen (estradiol) into the safer 2-hydroxyestrone (2OHE1) metabolite rather than the more harmful 16α-hydroxyestrone (16OHE1) 24. This process helps to reduce estrogen-fueled inflammation, alleviate pelvic pain, and improve irregular bleeding 25. Glucosinolates also increases liver detoxification, which helps clear the excess estrogen associated with estrogen dominance.
Irregular ovulation and high androgen levels contribute significantly to a state of estrogen dominance in individuals with PMOS. Ovulation is required to trigger the production of progesterone, so when ovulation is sporadic, progesterone plummets and creates a state of relative estrogen dominance. Excess androgens, particularly testosterone, are converted into excess estrogen in fat and other tissues, worsening the imbalance. While working on the underlying endocrine imbalances of low progesterone and high androgens, supporting estrogen detoxification with cruciferous vegetables can help favorably shift hormone balance away from a state of excess estrogen.
The Importance of Exercise in Managing PMOS
Increased movement through both cardiovascular exercise and resistance training is one of the most powerful tools for addressing the multiple features of PCOS. Exercise supports weight management, insulin sensitivity, mood and endocrine balance. Individuals with PCOS should strive for a minimum of 150 minutes of moderate intensity exercise or 75 minutes of higher intensity exercise per week, with two weight training sessions to build muscle and increase metabolic rate. 26
Clinical Takeaway
The most important takeaway here is that while a name change doesn’t change testing and treatment practices overnight, it does validate what women experiencing the condition have long known: this disease is not isolated to the ovaries. Polyendocrine Metabolic Ovarian Syndrome recognizes that this condition is a complex disorder requiring nutritional and lifestyle management across multiple systems, and offers a new opportunity for interventions to drastically improve the quality of life in women living with the disease.
Did you know WholisticMatters is powered by Standard Process? Learn more about Standard Process’ whole food-based nutrition philosophy.